Norah worked at CAFCL office for 15 years and I would see her around the office and through the different activities. When I heard that she had back surgery I was curious about her experience with her surgery and her recovery on her back! Thanks so much for your information and interview with your spinal stenosis. I hope people can learn about Norah and her experience.
Kelsey: What’s were your symptoms?
Norah: I was diagnosed with spinal stenosis about 10 years ago. It was very painful to walk.

Kelsey: Why did you need back surgery?
Norah: Vacuuming all sorts of different things shovelling snow was impossible and it got to the point where vacuuming or washing the floor was next to impossible.
Kelsey: How much pain were you in before your surgery, how long was recovery from the surgery?
Norah: The pain was pretty severe it went from my lower back down the back of my legs into my feet and up the front of my calves. The recovery from the surgery was four months. And up until the four months I didn’t know if I had done the right thing. I never had physio therapy before or after but after the four months. I was able to walk for a couple days and then a new pain started and I thought oh dear. I had an appointment with the surgeon and told him about the pain and he said unfortunately it probably is still part of the stenosis because it goes all the way up my spine. He told me in about six years I would probably need it again. I did not want to hear that but I’m so glad that I had the surgery.
Kelsey: If anyone else need this surgery, what would you say to them?
Norah: If anybody has it, I would say get the surgery it is changed my life. It’s given me back my life, I guess you could say I am able to walk now. I do an average of 10 to 15,000 steps a day which is about an hour and a half to two hours of walking.

Kelsey: What’s your hobbies?
Norah: As for hobbies I have all sorts of hobbies I love to paint, knit and crochet. I love to play cards with my good friends or family and grandkids.
Kelsey: Tell me about your childhood, where did you grow up? Do you have any siblings?
Norah: I grew up in Edmonton I was the youngest out of five kids, I had two sisters and two brothers.
Kelsey: How do I know you?
Norah: I worked at CAFCL for just about 15 years, and I met you through work at different events.

Kelsey: Do you have any memory of your parents?
Norah: I absolutely have great memories of my parents. They were the best parents any kid could ask for. We didn’t have a lot, but we always had a roof over our head and lots of food and clothes on our back. My parents have been gone for quite a while, my mom 15 years and my dad about 25 years now. They worked hard and the kitchen table always had lots of family and friends around it.
Kelsey: Did your family and friends give you support for your surgery?
Norah: My siblings and my kids gave me lots of support and my Friends were amazing.
Kelsey: What hobbies did you do as a child?
Norah: As a child I didn’t really have hobbies I babysat a lot I always loved kids.
Here is some information I found on the internet:
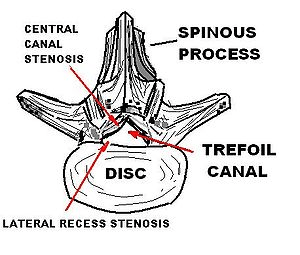
Spinal stenosis is an abnormal narrowing of the spinal canal or neural foramen that results in pressure on the spinal cord or nerve roots.[6] Symptoms may include pain, numbness, or weakness in the arms or legs.[1] Symptoms are typically gradual in onset and improve with bending forwards.[1] Severe symptoms may include loss of bladder control, loss of bowel control, or sexual dysfunction.[1
Causes may include osteoarthritis, rheumatoid arthritis, spinal tumors, trauma, Paget’s disease of the bone, scoliosis, spondylolisthesis, and the genetic condition achondroplasia.[3] It can be classified by the part of the spine affected into cervical, thoracic, and lumbar stenosis.[2] Lumbar stenosis is the most common, followed by cervical stenosis.[2] Diagnosis is generally based on symptoms and medical imaging.[4]
Treatment may involve medications, bracing, or surgery.[6] Medications may include NSAIDs, acetaminophen, or steroid injections.[7] Stretching and strengthening exercises may also be useful.[1] Limiting certain activities may be recommended.[6] Surgery is typically only done if other treatments are not effective, with the usual procedure being a decompressive laminectomy.[7]
Spinal stenosis occurs in as many as 8% of people.[4] It occurs most commonly in people over the age of 50.[8] Males and females are affected equally often.[9] The first modern description of the condition is from 1803 by Antoine Portal, and there is evidence of the condition dating back to Ancient Egypt.[10]